
A patient with abdominal pain
Abdominal pain results from GI disease and extra-intestinal conditions involving the genitourinary tract, abdominal wall, thorax, or spine.
There are four types of abdominal pain:
- Visceral. Gut organs are insensitive to stimuli such as burning and cutting but are sensitive to distension, contraction, twisting and stretching.
Pain from unpaired structures, such as the pancreas, is usually but not always felt in the midline. Pain from paired structures is felt on and radiates to the affected side, e.g. renal colic.
Pain arising from foregut structures (stomach, pancreas, liver and biliary system) is localized above the umbilicus.
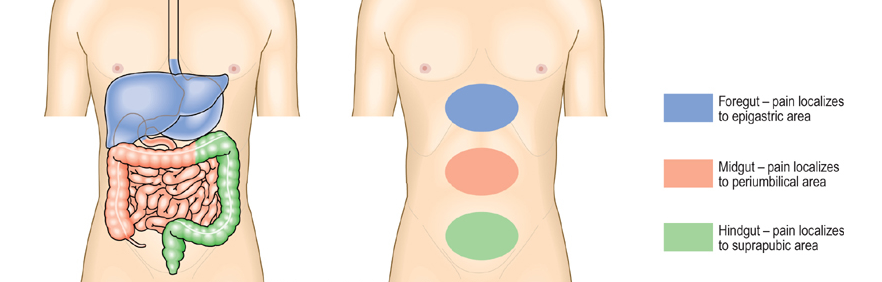
Pain arising from midgut structures (small intestine and colon up to right two-third of transverse colon) is felt around the umbilicus (periumbilical). If the parietal peritoneum is involved, the pain will localize to that area, e.g. right iliac fossa pain in acute appendicitis and in Crohn’s disease of the terminal ileum. Pain arising from hindgut structures (distal 1/3rd of transverse colon and rest of the colon) is localized below the umbilicus(suprapubic region).
- Parietal. The parietal peritoneum is innervated by somatic nerves, and its involvement by inflammation, infection or neoplasia causes sharp, well-localised and lateralised pain.
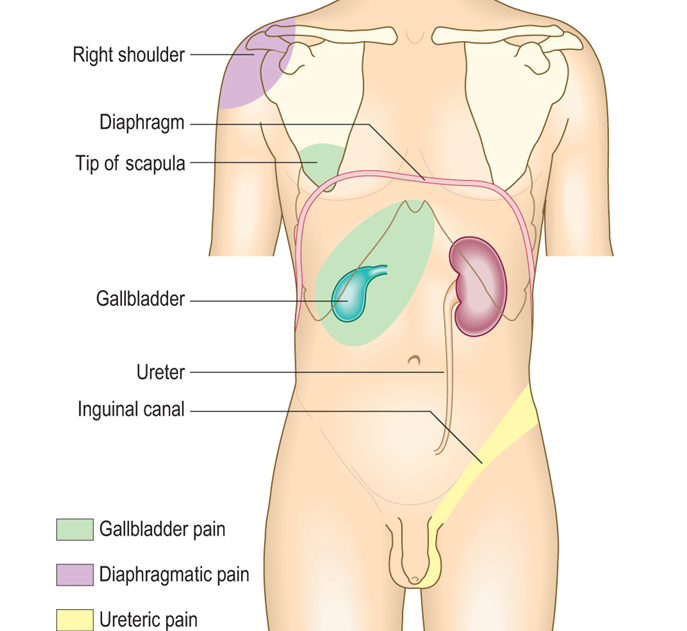
- Referred pain. Pain referred to the abdomen from the thorax, spine, or genitalia may prove a deficult diagnostic problem, because diseases of the upper part of the abdominal cavity such as acute cholecystitis or perforated ulcer are frequently associated with intrathoracic complications. To evaluate abdominal pain, the possibility of intrathoracic disease must be considered in every patient with abdominal pain, especially if the pain is in the upper part of the abdomen. Systematic questioning and examination directed toward detecting myocardial or pulmonary infarction, pneumonia, pericarditis, or esophageal disease (the intrathoracic diseases that most often masquerade as abdominal emergencies) will often provide sufficient clues to establish the proper diagnosis. In contrast to this, abdominal pain may refer to other part of the body (For example, gallbladder pain is referred to the back or shoulder tip.)
- Psychogenic. Cultural, emotional and psychosocial factors influence everyone’s experience of pain. In some patients, no organic cause can be found despite investigation, and psychogenic causes (depression or somatisation disorder) may be responsible.
Abdominal pain may present as acute abdominal pain or chronic/recurrent abdominal pain.
Acute abdominal pain (The acute abdomen) is a consequence of one or more pathological processes:
Inflammation: Pain develops gradually, usually over several hours. It is initially rather diffuse until the parietal peritoneum is involved, when it becomes localised. Movement exacerbates the pain; abdominal rigidity and guarding occur.
Inflammatory causes of acute abdominal pain are
- Appendicitis
- Diverticulitis
- Cholecystitis
- Pelvic inflammatory disease
- Pancreatitis
- Pyelonephritis
- Intra-abdominal abscess
Perforation. When a viscus perforates, pain starts abruptly; it is severe and leads to generalised peritonitis.
Perforation/rupture of
- Peptic ulcer
- Diverticular disease
- Ovarian cyst
- Aortic aneurysm
Obstruction. Pain is colicky, with spasms which cause the patient to writhe around and double up. Colicky pain which does not disappear between spasms suggests complicating inflammation.
Examples of obstruction are
- Intestinal obstruction
- Biliary colic
- Ureteric colic
Approach to the Patient with Abdominal Pain
A meticulously detailed history and physical examination are of the greatest importance in the evaluation of abdominal pain. A detailed history, with particular attention to the features of the pain and any associated symptoms is essential.
To assess abdominal pain, the points should be enquired
- Duration
- Site and radiation
- Severity
- Precipitating and relieving factors (food, drugs, alcohol, posture, movement, defecation)
- Nature (colicky, constant, sharp or dull, wakes patient at night)
- Pattern (intermittent or continuous)
- Associated features (vomiting, dyspepsia, altered bowel habit)
In cases of acute abdominal pain, a diagnosis is readily established in most instances, whereas success is not so frequent in patients with chronic pain such as IBS which is one of the most common causes of chronic abdominal pain and must always be kept in mind.
The location of the pain can assist in narrowing the differential diagnosis.
|
||||||||||||
|